The Honest Truth About Testosterone Replacement Therapy
What actually happens, who it’s really for, and what the marketing gets dangerously wrong.

A few years ago I quietly became a lesser version of myself.
Not dramatically sick. Just diminished. The man who used to run companies, train hard, and keep up with two young kids was being slowly replaced by someone who needed a fight to get through 4pm. Recovery from training got harder. Sleep got worse even though nothing about my life had obviously changed. The afternoon energy crash became routine. I’d hit 4pm and need to push through the rest of the day rather than drive through it.
I did what most men do. I assumed it was age. I told myself I needed to sleep more, train smarter, eat cleaner. I’d been doing all of those things already, but I doubled down. None of it moved the needle.
Eventually I did bloodwork. My total testosterone came back at 280 ng/dL. The clinical threshold for low testosterone is 300. I was below the floor. Not dramatically. Just enough to explain everything I was feeling.
That’s when the real education started.
The argument I want to make in this piece is simple: TRT is a legitimate medical treatment that has been both underprescribed by doctors and overhyped by influencers and telehealth clinics. The truth sits in the uncomfortable middle, and almost nobody is writing about it honestly.
What’s actually happening to men’s testosterone
Testosterone declines about 1 to 2% per year starting in your mid 30s. By the time most men hit 50, they’re 30 to 50% below their peak. This is normal biology and has been the case for as long as humans have been measured.
What’s not normal is how steeply baseline testosterone has fallen at the population level over the last several decades. Studies show today’s middle aged man has roughly 20% lower testosterone than a man of the same age in the 1980s. Younger men are starting from lower baselines than their fathers did. The decline curve is steepening.
The causes are debated but the suspects are familiar: obesity rates, sleep deprivation, chronic stress, sedentary lifestyles, environmental endocrine disruptors in everything from plastics to processed foods, and possibly the cumulative effect of modern life on the endocrine system. There’s no single villain. There are a hundred small ones.
The market response has been enormous. US testosterone prescriptions jumped from 7.3 million in 2019 to over 11 million by 2024. The global TRT market is over $2.1 billion. About 40% of men under 40 have expressed interest in testosterone optimisation. Around 14% have used TRT or are currently using it.
This is one of the fastest growing categories in men’s health, and like most fast growing categories, it’s attracted a lot of bad actors alongside the legitimate medicine.
What changed when I started TRT
I want to be honest about this part because most TRT content either oversells the transformation or dismisses it.
Within about six weeks of starting, my afternoon crashes disappeared. Not gradually. They just stopped. The fog I’d been pushing through for a year cleared. Recovery from training improved noticeably. My libido, which I’d assumed was just a function of being a married father in his forties, came back to something closer to what I remembered from my early thirties. My mood stabilised. The low grade irritability that had been there for months was gone.
The benefits below summarise what men on properly prescribed TRT typically experience, drawn from clinical literature and my own experience. Note the realistic timelines. Most of these are not immediate.
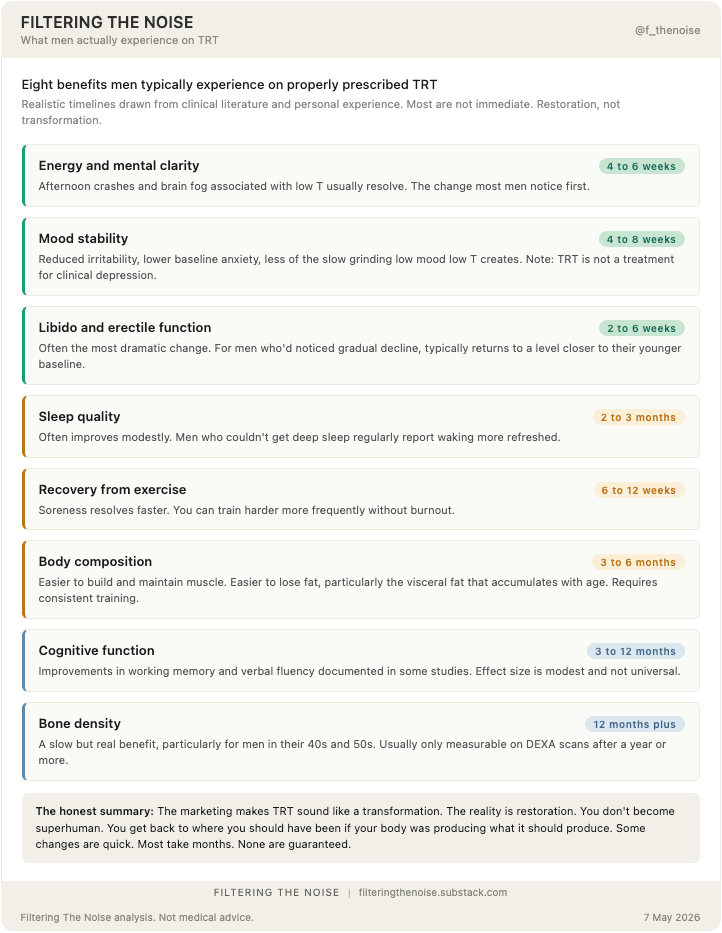
What didn’t happen: I didn’t become a different person. I didn’t suddenly want to enter Hyrox competitions. I didn’t develop superhuman energy. I didn’t start lifting weights I couldn’t lift before. The before and after wasn’t dramatic in the Instagram sense. It was just that the version of me I’d been losing came back online.
This is the experience most men on properly prescribed TRT actually report. The marketing makes it sound like a transformation. The reality is more like restoration. You’re not getting superhuman. You’re getting back to where you should have been if your body was producing what it should produce.
A small but important caveat. Some men start TRT and feel almost nothing. Their bloodwork improves but the symptoms don’t. This usually means the symptoms had a different cause (sleep, stress, thyroid, depression) and were never really about testosterone. If you start TRT and feel no better after 3 months with bloodwork in optimal range, you are probably solving the wrong problem.
The benefits also extend beyond the man taking the treatment. Partners often notice the changes before the man does. Mood stability returning, libido and intimacy returning, energy returning to evenings and weekends rather than being burned out at work. Marriages that had been quietly running on fumes find some of their spark again. This sounds like marketing copy and it isn’t. It’s a real downstream effect that nobody mentions in the clinical literature because it’s hard to measure.
Who actually needs TRT and who is being sold it
Here’s where the marketing wave has created a genuine problem.
Properly diagnosed hypogonadism (clinical low testosterone with symptoms) affects roughly 4 to 5 million American men. Fewer than 1 in 10 of these men are currently receiving treatment. That’s the underdiagnosis problem on one side.
On the other side, telehealth platforms are aggressively marketing TRT to men whose levels are within normal range but on the lower end. The pitch is “optimal” testosterone rather than “normal” testosterone. The implication is that even if you’re at 450 ng/dL (well within normal), you should be at 800 ng/dL because that’s where you’ll feel best.
This is a marketing argument dressed up as medicine.
The honest position is that genuine hypogonadism (under 300 ng/dL with symptoms) has well documented benefits from treatment. The case for TRT in men with normal testosterone (300 to 1,000 ng/dL) who simply want to feel better is much weaker, and the long term risks of supraphysiological testosterone levels are not well understood.
If your bloodwork comes back at 280 like mine did, with classic symptoms of low T, treatment is almost certainly worth considering. If your bloodwork comes back at 600 and you’re being told you need TRT to optimise, you’re probably being sold something.
The diagnosis problem
Most men who think they have low testosterone have never had proper diagnosis. They’ve maybe taken a single test, often at the wrong time of day, often without the supporting tests that actually tell you what’s happening.
Proper diagnosis requires:
Total testosterone measured between 7am and 10am (when levels are at their daily peak)
Free testosterone (the bioavailable portion, often more clinically relevant than total)
SHBG (sex hormone binding globulin) which determines how much of your testosterone is actually usable
LH and FSH (the pituitary hormones that signal whether the problem is in your testicles or your brain)
Estradiol (because testosterone converts to estrogen and the ratio matters)
Prolactin (high prolactin can suppress testosterone)
Thyroid panel (thyroid issues mimic low T symptoms)
A second test to confirm, ideally a few weeks apart
Telehealth platforms typically do total testosterone only, sometimes free testosterone. They don’t differentiate between primary hypogonadism (testicular failure), secondary hypogonadism (pituitary issue), or functional hypogonadism (lifestyle driven and potentially reversible). They prescribe TRT regardless.
This matters because some causes of low testosterone are reversible without TRT. Severe obesity. Untreated sleep apnea. Chronic alcohol use. Certain medications. Severe stress. If your low T is functional, fixing the underlying issue can restore your levels naturally. TRT in those cases treats the symptom while ignoring the cause.
If you’re considering TRT, find an endocrinologist or a urologist who specialises in male hormone health. Don’t start with a telehealth app.
What lifestyle alone can fix
Roughly 30% of men with low testosterone can get back to normal levels through lifestyle modification alone. The interventions that actually move the needle, in rough order of impact:
Weight loss for overweight men. Body fat converts testosterone to estrogen via aromatase. Obese men often see dramatic testosterone improvements with even modest weight loss.
Sleep. Most testosterone is produced during deep sleep. Untreated sleep apnea is a major hidden cause of low T in middle aged men.
Resistance training. The compound lifts (squats, deadlifts, bench, rows) genuinely move the needle. Cardio alone doesn’t.
Stress management. Chronic cortisol elevation suppresses testosterone. The interventions that work (sleep, exercise, meaningful relationships) are the same ones that improve everything else.
Reducing alcohol. Heavy drinking suppresses testosterone significantly. Even moderate drinking has measurable effects.
Vitamin D, zinc, magnesium. Correcting deficiencies works. Supplementing beyond sufficiency does not.
If you haven’t done these things consistently for at least six months, you don’t actually know whether you need TRT. You know you need to fix your life first.
What to avoid: the supplement aisle and the herbal optimisation crowd
Before we get to actual treatment options, a section on what doesn’t work, because there is an enormous amount of money being made selling men things that have almost no effect on testosterone.
Off the shelf “T boosters.” Walk into any GNC or Holland and Barrett and you’ll find dozens of products promising to boost testosterone. Most contain blends of zinc, magnesium, vitamin D, ashwagandha, fenugreek, D-aspartic acid, and other ingredients with names designed to sound scientific. The honest summary: if you’re deficient in zinc, magnesium, or vitamin D, correcting those deficiencies will help. If you’re not deficient, these products do essentially nothing.
Tongkat Ali and Fadogia Agrestis. This deserves its own treatment because the marketing has been particularly aggressive over the last two years, helped by Andrew Huberman discussing them on his podcast. The actual research is thin. Most positive studies on Tongkat are short, small, and conducted in specific populations (stressed men, infertile men, men with diagnosed deficiency). The Fadogia data is even thinner, mostly based on rodent studies that may not translate to humans.
I tried both for three months on the Momentous protocol that became popular in the optimisation space. I took the recommended doses consistently, didn’t change anything else, and ran proper bloodwork before and after. There was no meaningful change in my testosterone levels. None. The supplements cost roughly £80 a month combined. I wasted £240 finding out what the research already suggested: these are not testosterone boosters in any clinically meaningful sense for men with already adequate levels.
This doesn’t mean they do nothing. Tongkat may have mild stress and cortisol benefits. Fadogia may have some effect on libido in some men. But they are not a substitute for actual TRT in men with clinical deficiency, and they will not optimise testosterone in men with normal levels.
The “natural alternatives” framing more broadly. A lot of supplement marketing positions itself as a natural alternative to TRT for men who want to avoid pharmaceutical intervention. This framing is misleading. If you have clinical hypogonadism, no supplement protocol restores your testosterone to healthy levels. If you don’t have clinical hypogonadism, you don’t need a TRT alternative because you don’t need TRT.
The treatment options in 2026
If lifestyle isn’t enough and the diagnosis is confirmed, the treatment options have expanded meaningfully in the last few years. The infographic below summarises the five main routes with honest pros and cons for each.
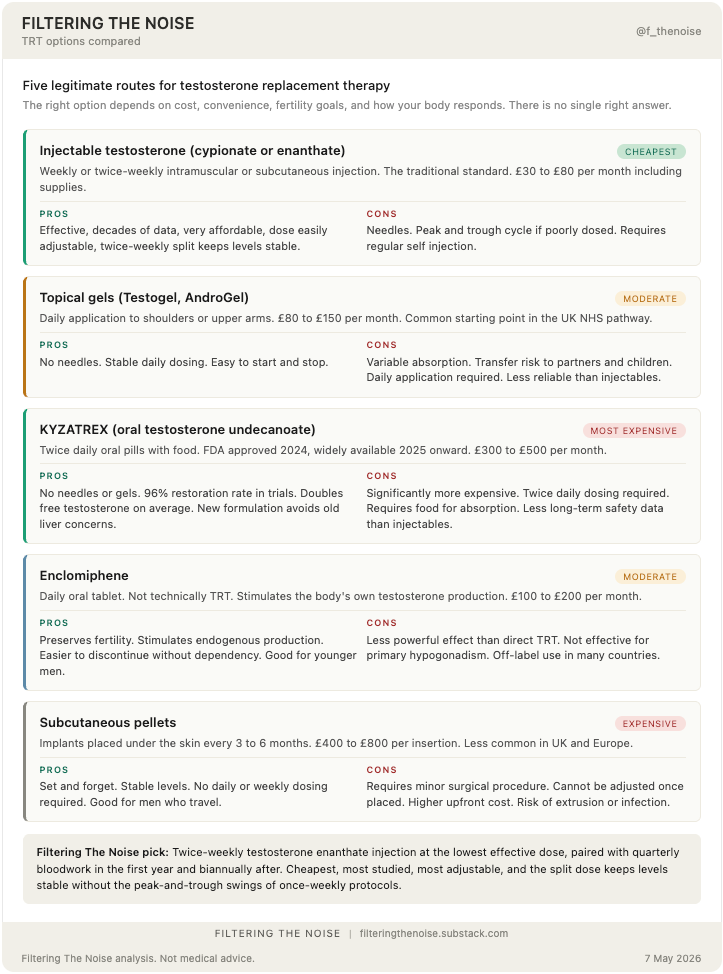
The right option depends on your priorities. If cost is a factor, injectables. If convenience is a factor, gels or KYZATREX. If fertility is a factor, enclomiphene. There isn’t a single right answer. What matters is that you choose with a doctor who actually monitors your response rather than just refilling a prescription.
The risks the evangelists don’t talk about enough
TRT is generally safe when prescribed and monitored properly. But “generally safe” is not the same as “no risks.”
Polycythemia. TRT increases red blood cell production. If left unmonitored, hematocrit can climb high enough to require blood donation or therapeutic phlebotomy. This is the most common side effect and needs regular bloodwork to catch.
Estradiol issues. Testosterone converts to estradiol. Some men aromatise too aggressively and end up with high estrogen, which causes water retention, mood issues, and gynecomastia. Some men over correct with aromatase inhibitors and crash their estradiol, which is its own problem.
Prostate and PSA. TRT does not cause prostate cancer, but it can accelerate growth of an existing tumour. Anyone starting TRT should have a baseline PSA test and digital rectal exam, and PSA should be monitored at least annually after that. The increased risk is small in absolute terms but the monitoring is non-negotiable.
Cardiovascular concerns. The FDA in 2024 concluded TRT does not increase cardiovascular risk based on the TRAVERSE trial. But that’s the population average. Individual cases of TRT contributing to cardiovascular events exist. Monitoring matters.
Fertility suppression. Traditional TRT shuts down your body’s own testosterone production and with it, sperm production. Most men recover fertility after stopping but not always. If you’re under 40 and want children, this matters more than any other risk. The two reasonable approaches are sperm banking before starting TRT (£300 to £600 in the UK for collection and the first year of storage) or using enclomiphene instead, which preserves fertility because it stimulates your own production rather than replacing it. Don’t let a clinic put you on TRT without addressing this if you might want children later.
Dependency. Once your body has been producing testosterone exogenously for years, restoring natural production is difficult and sometimes impossible. TRT is often a lifetime commitment. The marketing rarely emphasises this.
Coming off TRT. Related to dependency but worth saying directly. If you do decide to stop, you don’t just stop. You need a structured restart protocol using HCG and SERMs like clomiphene to encourage your testes to start producing again. The process takes 3 to 12 months and during that time you may feel worse than you did before TRT. Some men recover full natural function. Some don’t. This is one of the most underdiscussed parts of starting TRT and it should factor into your decision.
Cost. Properly managed TRT in the UK can cost £100 to £400 per month including bloodwork and consultations. In the US, it ranges from £30 (basic injectable) to £500+ (oral KYZATREX with full panel monitoring). Most insurance covers it for diagnosed hypogonadism but not for lifestyle optimisation.
What I actually do
I take 75mg of testosterone enanthate per week, split into two injections (37.5mg twice weekly). This is the lowest effective dose that resolved my symptoms while keeping hematocrit and estradiol in range. Many TRT clinics start men at 150mg or 200mg per week as a default, but more is not better. The right dose is the smallest one that gets you to feeling well with bloodwork in optimal range. The split dosing keeps blood levels more stable than once weekly injections and reduces the peak and trough effects.
I get bloodwork every three months for the first year and twice a year thereafter. I monitor hematocrit, estradiol, PSA, and lipid panel.
On injection method, the choice is between intramuscular (IM) into a muscle and subcutaneous (SubQ) into the fat layer just below the skin. I rotate between both depending on the day. SubQ into my shoulder when I want a quick, low pain injection with the smallest needle. IM into my glute (ventrogluteal site, the side of the hip rather than the upper outer buttock to avoid the sciatic nerve) when I want deeper absorption.
Within the TRT community specifically, shoulder SubQ has become one of the most common protocols because the absorption is consistent, the area has less subcutaneous fat than the abdomen so testosterone doesn’t pool, and it’s easy to self administer. Other common SubQ sites include the thigh and the love handle area. The abdomen is technically possible but most men on TRT find the shoulder or thigh works better.
For IM, the ventrogluteal hip area, the vastus lateralis (outer thigh), and the deltoid for smaller volumes are all valid. The traditional upper outer quadrant of the buttock (the dorsogluteal site) is generally avoided now because of nerve injury risk with repeated injections.
A few practical notes. Use the right needle gauge for the route, typically insulin needles for SubQ and 23 to 25 gauge for IM, and a separate 18 to 20 gauge for drawing the oil out of the vial. Always rotate sites to avoid scar tissue buildup.
The functional difference between SubQ and IM is mostly absorption rate. IM gives a slightly faster, slightly higher peak. SubQ gives a smoother, more consistent release. For most men on twice weekly protocols, either works equivalently and the choice comes down to comfort. SubQ uses a smaller, thinner needle and is significantly less painful. IM is what most men starting out are taught and works fine if rotated properly.
The total cost runs around £150 per month including private bloodwork and consultations. I consider it the highest ROI healthcare spending I do. To put that in context, that’s less than I wasted on Tongkat and Fadogia in three months for zero result. It’s a fraction of what telehealth optimisation clinics charge (often £300 to £500 per month for basic protocols with cursory bloodwork). And the return is not abstract. It’s hours of productive working time per week, mental clarity through afternoon meetings, energy left at the end of the day for my children, and proper recovery from training. For a 43 year old with another 40+ years of life ahead, paying to feel like myself rather than a slowly fading version is the most obvious purchase I make every month.
The honest conclusion
TRT is a legitimate medical treatment that has been overhyped by influencers and undertreated by traditional medicine. Both extremes are wrong.
If you’re in your 30s or 40s and you’re feeling the things I felt (the fog, the recovery issues, the energy crashes, the fading libido), get proper bloodwork done. Find an endocrinologist or urologist, not a telehealth app. Run the full panel I described. If your levels are clinically low and you have symptoms, treatment is genuinely worth considering.
If your levels are normal but you’ve been told you need optimisation, you’re probably being sold something. Fix the lifestyle factors first. Six months of consistent sleep, resistance training, stress management, and weight control will tell you whether your problem is biological or behavioural.
If you do start TRT, find a doctor who monitors properly and doesn’t just refill prescriptions. The treatment works when it’s done right. It causes problems when it isn’t.
The men telling you that TRT is a scam are wrong. The men telling you everyone over 30 should be on it are also wrong. The truth is the same as it usually is: a real medical treatment, helpful for the right people, harmful when applied indiscriminately, and currently being marketed in ways that obscure both realities.
If you’re in the right group, this can give you back years of your life. If you’re not, you’d be solving a problem you don’t have and creating ones you don’t need.
Get the bloodwork. Find a real doctor. Make an informed decision.
If this piece resonated with you, the single most helpful thing you can do is hit the like button and share it with anyone who might benefit from a clear honest take on this topic. Every share helps Substack surface the work to new readers, which is how this newsletter grows.
Reply to this email with your own experience or questions. I read everything and the strongest writing comes from honest exchange with people who’ve lived the questions I’m asking.
The hundred small ones framing is the part most population level testosterone coverage flattens entirely.
People hear the 20 percent generational drop and picture a single villain.
A hundred small inflows is a different argument and lands closer to how the EDC literature actually reads.
The Tongkat and Fadogia personal bloodwork is the cleanest version of run the test before you trust the marketing I've seen anyone publish.
Most men in the optimisation space never run the before and after themselves, and the supplement category survives on people who didn't.
The 280 to clinical 300 floor reframe is the part that should land hardest in the diagnosis section.
Most men assume below the floor means dramatic deficiency.
Just enough below to explain everything you were feeling is the much more common pattern, and almost nobody walks into a GP appointment expecting that number to matter.
For the lifestyle list you ranked, where would you put the personal care and household chemical inflow audit alongside weight, sleep, lifting, stress, alcohol, vitamin D?
The HERMOSA biomarker data sits inside the same reversibility window as the items you ranked, but the male side rarely gets a parallel checklist.
p.s. side project of mine, mangood.app, basically a scanner for hormone disrupting ingredients in everyday products tuned for men.
Sits next to the inflow audit that doesn't quite make the lifestyle list yet.
Still beta. Would value your eyes if you ever have a sec.